Diagnosing the Torn ACL in the Acute Knee
Introduction
Diagnosis of ACL Deficiency
Diagnosis in the acute setting is made by the history of mechanism and specific findings on examination. In the patient who complains of repeating episodes of giving way then there will often be found a history of an injury some months or years before associated with a significant downtime from sport and a persistent feeling of not trusting the knee on pivoting and turning.
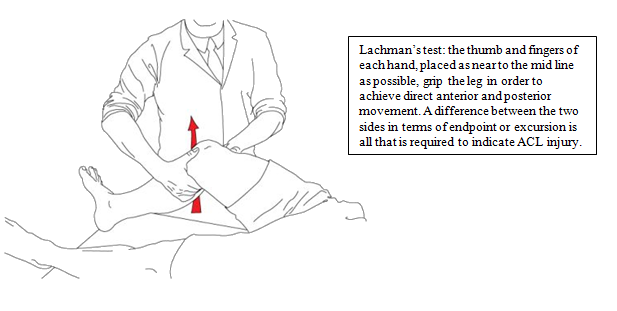
The main signs on examination are the positive Lachman’s test and pivot shift test, each described briefly below. See the document ‘History and Examination of the Knee’, available on www.timspalding.com, for more in-depth information regarding clinical assessment of the knee.
In the Lachman’s test the knee is held at 15° flexion and an anterior drawer made on the tibia against the femur sensing increased movement.
The pivot shift test is diagnostic of ACL rupture as it reproduces the patient’s sensation of the tibia jumping on the femur.
Obesity is one of the most common comorbidities in patients seen in the knee clinic. With obesity levels in the UK rising every year, over 50% of the population is set to be clinically obese by 2050. At such levels, it is projected that Obesity could cost the NHS nearly £50 billion per year.
The mechanical implications of obesity for the knee and other joints in the body are, perhaps, obvious. However, overloading is not the only way that obesity can affect the knee. The full range of issues associated with obesity can be grouped as follows:
- Mechanical factors
- Systemic factors
- Surgical factors
- Anaesthetic factors
Each of these areas is discussed briefly, below.
Mechanical Factors
The most recognised and well-studied association between obesity and knee pathology is that of osteoarthritis. Obese patients place increased stresses on their articular cartilage, which drives earlier onset and more rapid degenerative changes. Furthermore, there is a higher rate of varus alignment in the obese population, which places additional stress on the medial compartment of the knee joint.
Apart from osteoarthritis, a recent study has shown that obese patients are more likely to suffer multi-ligamentous knee injuries due to low energy mechanisms. Such injuries can be devastating for the function of the knee, particularly when considering the difficulties associated with surgery and obesity, which are discussed below.
Systemic factors
Overloading alone does not account for all of the increased morbidity associated with osteoarthritis in the obese population. Over recent years, it has become increasingly evident that adipose tissue has a role as an endocrine organ, producing a variety of hormones and biochemical factors that affect the function of a wide variety of systems in the body. Many of these chemicals – including chemokines, cytokines and adipokines – are pro-inflammatory and therefore exacerbate symptoms such as pain and swelling associated with arthritis. They are also thought to disrupt the delicate balance of anabolic and catabolic processes within joints, which can lead to increased degeneration of cartilage and other soft tissues. The role of adipose tissue helps explain why osteoarthritis of non load-bearing joints – e.g. in the hands and fingers – is also more common in obese patients.
Surgical factors
There are a number of ways in which obesity affects surgical procedures and outcomes. It should come as no surprise that procedure time is increased for obese patients, as is the overall length of stay in hospital. Obese patients are also likely to experience worse overall outcomes and satisfaction levels following their operation. For example, in total knee replacement surgery for normal weight population, around 90% of patients will be satisfied with the result. In the obese population, only 70% have a good outcome. At least part of the reason for this is increased rate of complications, such as delayed wound healing, more post-operative pain and increased rates of deep vein thrombosis.
Anaesthetic factors
In general, obesity is a risk factor for a number of systemic diseases, such as cardio-respiratory (eg. hypertension, heart failure), metabolic (eg. diabetes) and gastrointestinal conditions (eg. gastro-oesophageal reflux disease), all of which can have anaesthetic implications.
Specific difficulties that the anaesthetist may encounter include:
- airway problems associated with anatomical restrictions and sleep apnoea, which can also cause perioperative drowsiness, complicating assessment and treatment.
- Ventilation problems due to difficulty intubating the patient, reduced lung capacities and low chest wall compliance.
- Inaccurate blood pressure readings using normally available cuff sizes
- Unpredictable pharmacokinetics leading to unknown rates of drug elimination, etc.
- Loss of landmarks for regional anaesthesia
- More difficult venous access
The Good News
For the reasons outlined above, obese patients can experience dramatic improvements in their symptoms and response to treatment if they are able to lose weight. The effects of mechanical, systemic and other factors are additive, such that even a reduction of a few percent (5% – 10% is often targeted) can deliver significant benefits. The systemic effect of adipose tissue means that greater benefit is derived if weight loss can be achieved through reduction of body fat percentage, rather than loss of muscle. Studies have shown that good advice alone is not sufficient for successful weight loss – patients who are actively supported through the process tend to do much better. In cases of extreme obesity, patients may wish to consider other weight—loss options, such as bariatric surgery, before electing for orthopaedic surgery.
When dealing with the acutely injured knee, the detection of injury to the anterior cruciate ligament (ACL) is an essential part of the management aim. Most acute knee injuries will settle over time and patients will be tempted to return to sport. However, ruptures to the anterior cruciate ligament will result in a patient feeling perfectly stable on their knee while running in straight lines but they will be at risk of their knee giving way again if they try to pivot or twist on it. Subsequent episodes of giving way are likely to result in a tear to the meniscus (footballer’s cartilage) or damage to the articular cartilage. This second injury starts the downward spiral towards later degeneration in the knee.
It is for this reason that this section directs diagnosis towards excluding rupture of the anterior cruciate ligament.
Anatomy and Function of the ACL
The anterior cruciate ligament acts as the main link mechanism between the tibia and the femur, preventing anterior movement of the tibia on the femur. When pivoting therefore, the femur and tibia usually act as one but without the ACL the tibia is allowed to jump forward and back again creating the sensation of the knee giving way.
Differential Diagnosis
Injury to the ACL is, of course, only one of the potential diagnoses that need to be considered in the acutely injured knee. Others include:
- Meniscal tear
- Collateral ligament tear
- Patella dislocation
- Ruptured posterior cruciate ligament
- Simple knee sprain
The key features of each of these injuries are described below.
a. ACL rupture.
The mechanism of injury is usually a non-contact situation associated with rapid deceleration. The patient may describe a pop or a snapping sound and they are usually unable to play on. If they do then the knee gives way again. Swelling appears within four hours or so and diagnosis is made on the Lachman and pivot shift test.
b. Torn meniscus.
The mechanism to tear the meniscus is usually a weight bearing twisting injury, often associated with a tearing sensation. The knee may be locked as the meniscus obstructs full extension of the joint. Swelling appears more delayed than after ACL rupture, often after four hours and usually overnight. Diagnosis is made by eliciting tenderness on the joint line.
c. Collateral ligament injury.
The mechanism for injury to the lateral collateral ligament or medial collateral ligament is a blow from the side of the knee resulting in localised pain on the attachment points to the ligament with tenderness over the affected femoral condyle. Swelling is variable and is usually outside of the joint.
d. Patella dislocation.
Patella dislocation is often difficult to elicit and it depends on the history from the patient who may describe a sensation of their knee dislocating. This often has to be specifically asked for. Tenderness is usually felt around the medial para-patella border, immediately adjacent to the patella. The patient would be reluctant to allow their patella to be pushed laterally.
e. Posterior cruciate ligament.
The PCL is injured by a direct blow to the anterior part of the tibia driving the tibia posteriorly or by a significant hyperextension mechanism. The symptoms will be variable but the main sign is posterior sag of the tibia on the femur when viewed from the side (sag sign).
Management Principles
The main principle for managing the acute knee is to attempt to assess the knee in the acute setting and then to immobilise the joint with a supportive bandage or splint for 2 or 3 days prior to further examination.
Ice may be applied to try and reduce pain and swelling. Aspiration for analgesia is generally reserved for the severely tense knee which is very painful due to the tension. Such a knee may benefit from removing the bleeding from the joint.
After a few days rest mobilisation is attempted aiming for gradual increase in range of movement while re-evaluating the knee at various time intervals over the subsequent six weeks.
This management plan is based on the principle that most minor injuries will settle by six weeks and that some meniscal tears can heal without needing urgent intervention.
URGENT REFERAL TO HOSPITAL: The main indication for referral to hospital acutely is for a locked knee (where the leg will not go fully straight) and the very unstable knee where there is possibly complete rupture of the medial collateral ligament.
ACL Management Plan
Management of the sportsman with rupture to the anterior cruciate ligament is based on multiple factors. The principle is early diagnosis in order to prevent the second episode of giving way that may subsequently damage the meniscus or articular surface. Early rehabilitation following injury is directed at regaining full range of movement, balance control and re-learning confidence in the knee.
A decision is made on the level of sporting aims and, if considered appropriate, then reconstruction surgery is performed after the acute inflammation has settled. This is usually at six to twelve weeks post injury allowing a return to contact sport at six to nine months.
Joint Surface Damage
We know that the time interval between injury and reconstruction increases the risk of articular cartilage damage and this knowledge argues in favour of early reconstruction of the anterior cruciate ligament before any repeated episodes of giving way have caused damage to the joint surface.
The area of articular surface damage is related to the time since injury and also to the state of the meniscus. The area is increased six fold if it is more than two years since injury and three fold if associated with loss of the meniscus.
Ten years following ACL rupture the incidence of degenerative change seen on the x-ray is only 10% in the presence of a normal meniscus but is up to 60% if the whole meniscus has been removed.
Surgical Reconstruction of ACL Injury
ACL reconstruction is now a reliable procedure with over 9 out of 10 reconstructions resulting in a normal or nearly normal knee. The aim of reconstruction is to improve function and it is not appropriate to say that reconstruction actually prevents arthritis in the long term. It is known that arthritis following the ACL is related to the secondary injury and has a higher prevalence where the meniscus or articular cartilage has been damaged.
Repeated giving way of the knee results in increased chance of injury to the meniscus and to shear injury on the articular surface. There is a 45% chance of tearing the meniscus over a three to five year period if an individual continues to play sport with an unstable knee.
The best results from ACL reconstruction are seen when there has been no previous tear to the meniscus or damage to the articular surface.
Surgical Techniques
Currently the surgical technique involves reconstituting the cruciate ligaments using the hamstrings (semi tendinosis and gracilis tendons) harvested through a small incision. The newest techniques focus on inserting the graft in the true anatomical position and recent work at UHCW and published in the Journal of Arthroscopy has helped improve the accuracy of the surgery.
Occasionally the central third of the patella tendon (10mm wide strip of the patella tendon with bone from the patella and tibial tubercle) is used for the graft
In the operation the new tissue is fashioned into an appropriate size and tunnels are drilled into the femur and then through the tibia and the operation is assisted by use of the arthroscope. For information on other arthroscopic procedures, see Appendix A.
The new graft is held in placed using either a metal ‘endobutton’ device on the femur and a tensioner system with absorbable screw on the tibial side. When the Patella tendon graft is used this is held in place with bioabsorbable screws.
Post Operative Rehabilitation
Following ACL reconstruction patients are discharged home on the day following surgery, walking with two crutches with their leg in a light tubigrip support. No braces are used.
Patient should expect to have a comfortable 90° bend by two weeks and to be back to activities of daily living by four weeks.
Driving is allowed at three to four weeks and this is often the time for return to deskwork.
Standing work is usually tolerated after six weeks whereas heavy manual work is generally not expected for three months. Return to scaffolding, ladders or roof work is expected at four months.
As regards return to sport, running is started at two to three months but pivoting is not allowed for four months. Contact sport training is commenced at six months and patients could usually be back to full sporting activity at around nine months.
Summary
When faced with the acutely injured knee, our aim is to repeatedly assess the knee with a view to making an early diagnosis of rupture of the anterior cruciate ligament. The principle is to try and prevent repeated giving way and it may take repeated examination to detect any laxity and looseness in the knee. Patients should be referred for specialist opinion via A&E early if there is an acutely locked knee or significant ligament laxity is detected.
If symptoms do not settle over the first six weeks then patients should be referred before they recommence sport, so that rupture of the ACL may be confidently excluded.
ACL reconstruction is now a procedure with greater than 90% success and late diagnosis of ACL injury is associated with a worse outcome.